Retatrutide and Semaglutide are two widely discussed peptides in metabolic health research. Learn the key differences in their mechanisms, research focus, and potential benefits for weight management and glucose regulation in this comprehensive comparison guide.
Semaglutide has transformed the treatment landscape for obesity and type 2 diabetes in the UK. Available in the UK as Ozempic (for diabetes) and Wegovy (for weight management), it has become one of the most prescribed and discussed pharmacological compounds of recent years.
Retatrutide is now emerging as a potential successor — or complement — to semaglutide in the research and clinical pipeline. Understanding the key differences between these two compounds is essential for UK researchers evaluating either one for investigative work.
This comparison focuses on mechanism, Phase 2/3 research data, and research relevance. It is not a clinical recommendation.
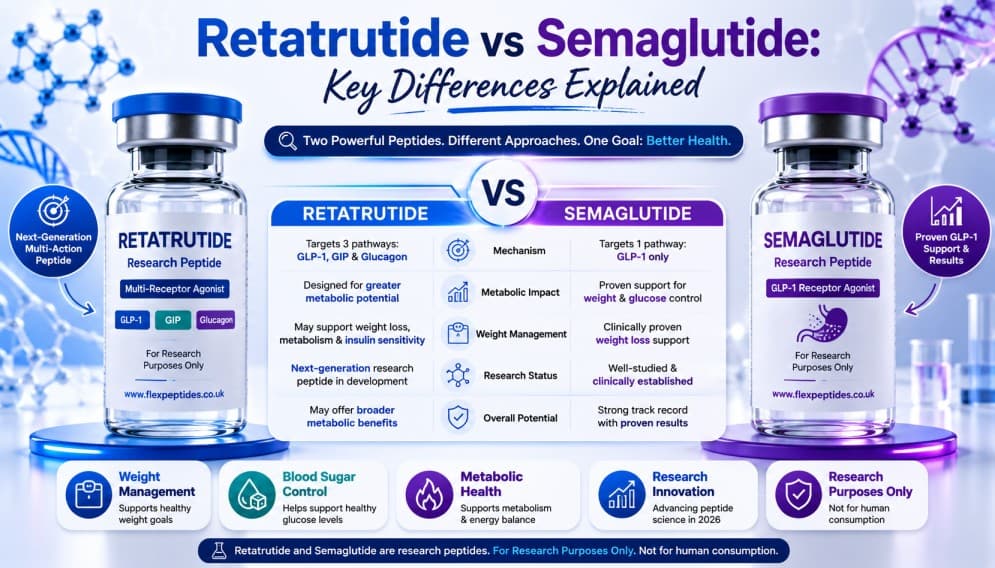
At a Glance: The Core Difference
The fundamental difference between semaglutide and retatrutide is their receptor profile. Semaglutide is a GLP-1 receptor agonist — it acts on one receptor. Retatrutide is a GLP-1, GIP, and GCG triple receptor agonist — it acts on three. Every other difference in their research profiles flows from this distinction.
Feature Semaglutide Retatrutide
Receptor targets GLP-1 only GLP-1 + GIP + GCG
Class Single agonist Triple agonist
Development stage (2026) Approved (UK) Phase 3
UK brand name Ozempic / Wegovy None (investigational)
MHRA approval Yes (licensed uses) No
Primary research focus T2D, obesity Obesity, NASH, T2D
Mechanism Comparison
How Semaglutide Works
Semaglutide mimics the action of GLP-1, a hormone released from the gut after eating. It stimulates insulin secretion in a glucose-dependent manner, suppresses glucagon secretion, slows gastric emptying, and reduces appetite through central nervous system signalling. Its once-weekly dosing format and long half-life (approximately seven days) contribute to its clinical convenience.
How Retatrutide Differs
Retatrutide activates GLP-1 receptors in the same way as semaglutide, but adds two additional layers of action. GIP receptor activation enhances insulin response and appears to reduce GI side effects. Glucagon receptor activation — the component unique among currently approved or late-stage drugs — appears to increase energy expenditure and enhance hepatic fat clearance. The theoretical result is a compound that achieves appetite suppression (GLP-1), enhanced insulin response (GIP), and boosted fat burning (GCG) simultaneously.
Research Data: What the Evidence Shows
Semaglutide — Established Evidence Base
Semaglutide has one of the most robust evidence bases of any metabolic compound in history. The SUSTAIN trials (type 2 diabetes) and STEP trials (obesity) demonstrated consistent, reproducible results across diverse populations, including meaningful reductions in body weight and, notably, cardiovascular risk reduction in the SUSTAIN-6 and SELECT trials.
Retatrutide — Emerging Evidence
Retatrutide's Phase 2 data, published in 2023, showed body weight reductions at 48 weeks that appeared to exceed benchmark results from semaglutide trials in comparable populations. However, these are not head-to-head comparisons — differences in trial design, population, and duration make direct comparison complex. Phase 3 data from the TRIUMPH programme will provide more definitive insights.
Side Effect Profiles
Both semaglutide and retatrutide share the most common adverse effect profile of the GLP-1 agonist class: nausea, vomiting, diarrhoea, and constipation, typically most prominent at initiation or dose escalation and tending to diminish over time. Retatrutide's GIP component may attenuate some of these GI effects, based on preclinical reasoning and early trial observations. However, formal comparative safety data from head-to-head studies is not yet available.
Research Use in the UK
In the UK, semaglutide is available as a licensed medicine through prescription and is also used as a reference compound in metabolic research. Retatrutide occupies the research peptide category — it can be sourced through specialist UK suppliers with appropriate documentation for use in legitimate investigative work.
For researchers designing studies that seek to understand differences between GLP-1 only, GLP-1/GIP dual, or GLP-1/GIP/GCG triple agonism, both compounds offer distinct mechanistic profiles worth investigating.
⚠️ Semaglutide requires a valid UK prescription for clinical use. Retatrutide is a research compound not currently approved for any licensed clinical use in the UK.
Summary: Why Researchers Choose One Over the Other
Researchers choose semaglutide as an established reference compound with a deep evidence base, ideal for head-to-head comparison studies, available in licensed clinical form for appropriate patient populations. Researchers choose retatrutide when investigating the incremental effects of GIP and/or GCG receptor activation beyond GLP-1 agonism, exploring triple agonism as a research framework, or studying mechanisms of hepatic fat metabolism, energy expenditure, or appetite regulation from a novel angle.
Read More in This Series
→ Retatrutide UK: Complete Guide | FlexPeptides
→ Retatrutide vs Tirzepatide: Which Research Peptide Is More Popular? | FlexPeptides
→ Retatrutide vs Other Metabolic Research Peptides | FlexPeptides
→ Retatrutide Research: Current Scientific Interest in 2026 | FlexPeptides
Disclaimer: This article is for educational and research purposes only. Neither semaglutide nor retatrutide should be used for self-administration. Consult a licensed UK medical professional for any clinical application.